IHTSDO-444 (artf222572) Rework hierarchy Injury of body cavity
Taken from a word document. Source has not be uploaded to confluence.
SNOMED CT Content Improvement Project Inception phase | ||
Project ID: artf222572 Topic: Rework hierarchy Injury of body cavity
| ||
Date | December 2016
| |
Version | 0.4 | |
|
|
|

Amendment History
Version | Date | Editor | Comments |
0.1 | 20150808 | ‘Ismat MS | First draft |
0.2 | 20150822 | 'Ismat MS | Revised |
0.3 | Sept 2016 | 'Ismat | Revised |
0.4 | Dec 2016 | 'Ismat | Revised |
Review Timetable
Review date | Responsible owner | Comments |
25/11/2016 | Yongsheng Gao | Comments provided for revision |
30/03/2017 | Yongsheng Gao | Appproved |
© International Health Terminology Standards Development Organisation 2012. All rights reserved.
SNOMED CT® was originally created by the College of American Pathologists.
This document forms part of the International Release of SNOMED CT® distributed by the International Health Terminology Standards Development Organisation (IHTSDO), and is subject to the IHTSDO’s SNOMED CT® Affiliate Licence. Details of the SNOMED CT® Affiliate Licence may be found at http://www.ihtsdo.org/our-standards/licensing/.
No part of this document may be reproduced or transmitted in any form or by any means, or stored in any kind of retrieval system, except by an Affiliate of the IHTSDO in accordance with the SNOMED CT® Affiliate Licence. Any modification of this document (including without limitation the removal or modification of this notice) is prohibited without the express written permission of the IHTSDO.
Any copy of this document that is not obtained directly from the IHTSDO [or a Member of the IHTSDO] is not controlled by the IHTSDO, and may have been modified and may be out of date. Any recipient of this document who has received it by other means is encouraged to obtain a copy directly from the IHTSDO [or a Member of the IHTSDO. Details of the Members of the IHTSDO may be found at http://www.ihtsdo.org/members/].
- 1 1 Glossary
- 2 3 Statement of the problem or need
- 2.1 3.1 Summary of problem or need, as reported
- 2.2 3.2 Summary of requested solution
- 2.3 3.3 Statement of problem as understood
- 2.4 3.4 Detailed analysis of reported problem, including background
- 2.5 3.5 Subsidiary and interrelated problems
- 2.5.1 3.5.1 Review the definition description for |Traumatic injury (disorder)|
- 2.5.2 3.5.2 Review |Injury of internal organ (disorder)| as a child concept for |Injury of body cavity (disorder)|
- 2.5.3 3.5.3 Confusing FSN for |Injury of body cavity (disorder)| and |Body cavity structure (body structure)|
- 3 4 Risks / Benefits
- 4 5 Requirements: criteria for success and completion
- 5 6 Outline Possible Technical Approaches and Concept Model
- 6 7 Indicative Project Plan
1 Glossary
1.1 Domain Terms
Navigational concept | SNOMED CT Glossary: A hierarchical view of a set of SNOMED CT concepts that is intended to assist navigation at the user interface . Note: There are several differences between navigation hierarchies and the formal subtype hierarchy :
|
Navigational link | An association between two Concepts that supports Navigation between Concepts. Such links may involve one of more Navigational Concept but are not required to. Navigation Links generate a hierarchy which has three distinct differences from the subtype hierarchy defined by | is a | Relationship. A navigational hierarchy:
Alternative Navigation Subsets may be specified and applied to vary the navigation hierarchy to meet the needs of particular groups of users. |
Navigational subset | A Subset that specifies sets of Navigation Links between Concepts together with a display sort order. The set of Navigational Links in a Navigational Subset encodes an arbitrarily defined mono– or polyhierarchical organisation of the concepts referenced within. The set of concepts so organised may be any mixture of active and inactive concepts, and may or may not include any Navigational Concepts. The semantics of Navigation Links between concept pairs need be neither explicit nor constant across the Navigational Subset as a whole, though the mechanism does not preclude its use to encode a formally specified and computable hierarchy. |
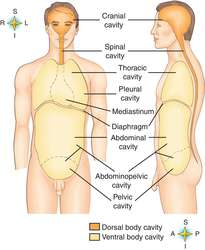
Body cavity |
Synonym(s): celom (2) , celoma, coelom (1)
Reference: Farlex Partner Medical Dictionary (2012). Retrieved September 15 2016 from http://medical-dictionary.thefreedictionary.com/body+cavity
2. Any of the spaces in the human body that contain organs.
Reference: Mosby's Medical Dictionary, 9th Edition (2009). Retrieved September 15 2016 from http://medical-dictionary.thefreedictionary.com/body+cavity
|